


AESTHETIC PLASTIC
RECONSTRUCTIVE
SURGERY
SEBASTIEN GARSON M.D
EARS
This fact sheet was developed under the aegis of the French Society of Plastic Reconstructive and Aesthetic Surgery (SOF.CPRE) as an addition to your initial consultation, to try to answer all the questions you can ask yourself if you plan to use surgery baldness. The purpose of this document is to provide you with all the necessary and essential elements of information to help you make your decision with full knowledge of the facts. Also you is it advisable to read with the greatest attention.
• DEFINITION OBJECTIVES AND PRINCIPLES
The correction of protruding ears requires surgery, called "otoplasty" to reshape the pavilions considered excessively visibles.L operation is usually performed on both ears, but can sometimes be unilateral. Otoplasty proposes to correct cartilage abnormalities present at the pinna and responsible for its appearance "off". We can roughly distinguish three types of defects that are often more or less associated with each other:
• excessive angulation between the external ear and skull realizing the true "detachment" (Helix Valgus).
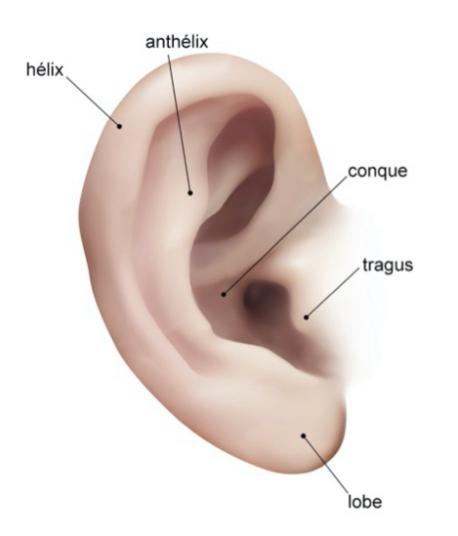
• Excessive Size cartilage of the concha (see diagram) projecting ear forward, which accentuates the look off (enlarged concha).
• A lack of kinking usual reliefs cartilage that causes the pinna was too smooth, like "deshirred" (default plication antihelical).
The intervention aims to permanently correct these defects by reshaping the cartilage, so get ears "glued together", symmetrical, size and natural appearance, thereby ending teasing and other derogatory remarks may be cause psychological difficulties or school conflicts. Otoplasty can be performed in adults or adolescents, but most of the time the correction is considered as a child where she can be performed from the age of 7, when the child complains its appearance and suffers.
• BEFORE THE OPERATION
A careful examination of the ears has been made by the surgeon to analyze the modifications.
A typical pre-operative assessment is done in accordance with If other than purely local anesthesia, the anesthesiologist will be seen in consultation at least 48 hours before surgery. No medication containing aspirin should be taken within 10 days before surgery.
For boys, a very short hair cut is desirable (For girls, a ponytail is welcome).
The head and the hair will be carefully washed the day before the operation.
Depending on the type of anesthesia, it will be fasting (nothing to eat or drink) 6 hours before surgery.
• TYPE OF ANESTHESIA AND CONDITIONS OF INTERVENTION
Type of anesthesia:
Three methods are possible:
Local anesthesia pure analgesic where a product is injected locally to ensure insensitivity ears.
Local anesthesia depth by tranquilizers administered intravenously (anesthesia "vigil").
classic General anesthesia, in which you sleep completely.
The choice between these techniques is the result of a discussion between you, the surgeon and the anesthetist.
Terms of admission:
Usually the procedure is done in "outpatient", that is to say, on an outpatient basis, with a registered the same day after a few hours of monitoring output.
However, in some cases, a short hospital stay may be preferred. The input is then carried out in the morning (or sometimes the day before in the afternoon) and the output is usually permitted the next day.
• INTERVENTION
Each surgeon adopts a technique of its own and it adapts to each case to obtain the best results. However, it may hold common basic principles:
Incisions:
Usually, they are located only in the retroauricular sulcus, that is to say in the natural crease behind the ear.
In some cases, additional small incisions will be made in front of the flag, but they will be hidden in natural folds. It should be noted that at no time the hair is cut.
Dissection:
The skin is then peeled off as needed to access the cartilage.
Cartilage remodeling:
The idea is to recreate or improve the natural contours by refining and kink, possibly maintained by thin deep sutures. Sometimes sections or cartilage resection is needed. Finally, the flag is returned in good position relative to the skull and fixed by deep points.
Sutures:
Classically, absorbable son are used, otherwise they will be removed to the 10th day.
Dressing:
It is made with an elastic band around the head to keep the ears in a good position. Depending on the surgeon and the importance of correcting defects, bilateral otoplasty can take half an hour to an hour and a half.

AFTER THE INTERVENTION: THE OPERATING SUITES
The pain is usually mild and, if necessary, fought by an analgesic and anti-inflammatory treatment. Otherwise, a consulting surgeon or
his team needed. The first big bandage will be removed between the 2nd and 5th
postoperative day. Beyond that, it is usually replaced by a lighter bandage for a few days. The ears will then appear swollen, with reliefs
masked by edema (swelling). Blue more or less important are sometimes present. This potential aspect should not worry: it is only temporary and does not compromise
absolutely not the final result.
A band of restraint and protection (type "banner tennis") must be worn night and day for fifteen
days, and then only at night for a few weeks. During this period, physical or sports activities with risk of contact should be avoided.
Exposure to cold is not recommended for at least two months because of the risk of frostbite because of the transient decrease in the sensitivity of the ear.
• THE RESULT
Within one to two months is necessary to assess the outcome. This is the time required for the tissues are relaxed and all of edema has evaporated, leaving clearly show the contours of the ear. After this time, only the scars will still be a little pink and hardened before fading.
The intervention will most often been effective in correcting anomalies and get ears normally positioned and oriented, although Plicata symmetrical, size and natural appearance, not bloated.
In most cases, the results are final. However, a recurrence of detachment (partial principle) may possibly occur in the medium term, which then require a small reoperation.
Overall, this simple intervention principle and its realization can usually effectively correct the unsightly appearance that constitute the protruding ears which are the subject, particularly in the school setting, frequent teasing or disparaging remarks may be behind school conflicts or psychological difficulties.
• FAULTS OF THE RESULT
They may occur secondarily, for example due to unexpected reactions or scar tissue unusual phenomena. Thus we can sometimes observe a slight asymmetry between the two ears, small irregularities reliefs or kinking too prominent, a narrowing of the orifice of the ear canal, or a deep perception son.
These small defects, where they exist, are usually mild and do not attract attention. However, if they are still available at a small "touch" that will mostly under local anesthesia.
• POSSIBLE COMPLICATIONS
Otoplasty, although carried out mainly for aesthetic reasons, are nevertheless a real surgery, which involves risks
any medical procedure, however small it may be. We must distinguish the complications of anesthesia and those related to the surgery.
For anesthesia, during the consultation, the anesthetist inform himself the patient anesthetic risks. You should know that anesthesia in the body sometimes unpredictable, and more or less easy to control: the fact of using a fully qualified anesthetist, working in a surgical context that the risks have become statistically almost negligible. You should know, indeed, that the techniques, anesthetics and monitoring methods have made tremendous progress over the past twenty years, providing maximum security, especially when the operation is performed outside of the emergency and in a healthy person.
Regarding surgery: choosing a qualified and competent plastic surgeon, trained in this type of surgery, you limit these risks, without removing them completely. Fortunately, real complications are rare after otoplasty performed in the rules. In practice, the vast majority of happens without any problems and patients are fully satisfied with their results.
However, despite their rarity, you should be aware of possible complications:
postoperative bleeding: is it more important than a blood stain on the dressing (which has nothing to worry about), this may warrant further surgery to stop the bleeding at its source. Blood may also not externalize and give rise to a hematoma it is often preferable to evacuate.
skin necrosis: Exceptional, it sometimes occurs due to disturbance of traffic on the thin skin of the front of the house, next to a cartilaginous terrain. Healing occurs in rule through local dressings leaving a small scar.
Abnormal Scars: despite all the attention paid to the implementation of sutures, scars located behind the pinna may be the seat of inflammation and hypertrophy embarrassing, or even a "keloid" evolution (sustainability of scar hypertrophy) whose treatment is difficult.
In total there should not overstate the risks, but just be aware that surgery, even apparently simple, always has
a small share of hazards. The use of a qualified Plastic Surgeon ensures that it has the training and skill required to avoid these complications, or effectively treat the case
appropriate.
These are the pieces of information that we wanted to bring you in addition to the consultation. We recommend that you keep this document, read it again after the consultation and reflect "a clear head." This reflection may raise new questions for which you wait for additional information. We are available to talk during the next consultation, or by phone, or even on the day of surgery when we meet in any way before anesthesia.
CONTACT
Contact Us
Phone : + 33344282959
Address:
7 impasse de la Passerelle 60300 SENLIS
France
Copyright SELARL Dr Garson Pages d'information- Crédits photos : Dr Garson / Libre de droits - Mentions légales
Ce site utilise des cookies à des fins statistiques - Pour en savoir plus, cliquez ICI.
SITE RÉALISÉ AVEC WEBACAPPELLA RESPONSIVE
